Every year there are 45,000 cases of osteoporotic vertebral fractures in Italy, and there are now 15,000 hospitalizations per year for osteoporotic, traumatic or neoplastic vertebral fracture. Osteoporotic vertebral fractures constitute one of the most frequent manifestations of disease, often the cause of disabling pain which force the patient to immobility, with all the consequences of prolonged bedding (thrombophlebitis, phlebothrombosis, bedsores) and to the use of rigid restraint busts often maltolerant, especially by the patient of III age and with cardiorespiratory problems.
Fractures affecting patients with a T-score of Bone Mineralometry (MOC) lower than -2.5 are particularly frequent, and in patients who have used cortisone for a long time for chronic inflammatory diseases. Tumor vertebral fractures are unfortunately a of the most frequent complications of primary (born directly into the spine) or secondary (metastasis) tumors. Vertebrae can also be affected by various types of primary cancer, such as multiple myeloma, plasmacytoma, lymphoma, expansive angioma, osteoblastomas, sarcomas, etc.) or metastasis (usually from breast, lung, prostate and gastrointestinal carcinoma). , with the new methods of vertebral "remodeling" guided CT ("remodeling" or vertebral remodeling), exceptions or limits to the percutaneous reconstruction of a vertebra and if the intervention is conducted with a CT guide, the operating risks are practically canceled, in accordance with as demonstrated by the relevant scientific literature.
The Vertebral Reconstruction and / or Remodeling consists in the introduction, through a needle cannula, of a special "cement" which solidifies in a few minutes eliminating the risk of vertebral collapse in a vertebral body fractured by traumatic event, frailized by osteoporosis or destroyed by cancer. It is also possible, in case of traumatic fractures with severe deformation of the vertebral body, to re-expand the vertebra thanks to multiple systems (intravertebral stents, other devices for vertebral re-expansion) to restore a vertebral morphology as close as possible to the physiological data. Finally, new substances ("osteoinductors") capable of stimulating and accelerating vertebral bone regrowth, which will constitute the future of repairing a vertebral fracture, are currently being studied.
The most common techniques possible today with CT guidance are:
Examples of vertebral reconstruction with percutaneous guided CT Vertebroplasty technique
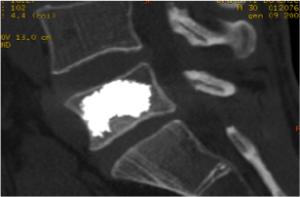
Example 1
Vertebral body reconstruction due to L5 vertebra fracture. The appreciable substance with an intense white in the image is Polymethylmethacrylate ("cement") inside the vertebral body previously suffering from vertebral fracture.

Example 2
Reconstruction of multiple fractures: the operation can also be performed simultaneously in multiple vertebral bodies during the same session, in patients suffering from multiple vertebral fractures.

Example 3
Spontaneous re-expansion of fractured and necrotic vertebra (Kummel s.) After introduction of particularly viscous cement. The height of the vertebra after the intervention (images below) appears significantly increased compared to that before the intervention (images above)
The sacred bone is often affected by fractures, not necessarily tumoral but also of a simple osteoporotic nature: unfortunately the fractures of the sacred bone are often invisible both to a simple radiographic examination and a CT scan, with consequent recognition of the same. Sacral fractures at an early stage are only appreciable on an MRI examination or a bone scan.
Examples of sacral reconstruction with percutaneous guided CT Sacroplasty technique.
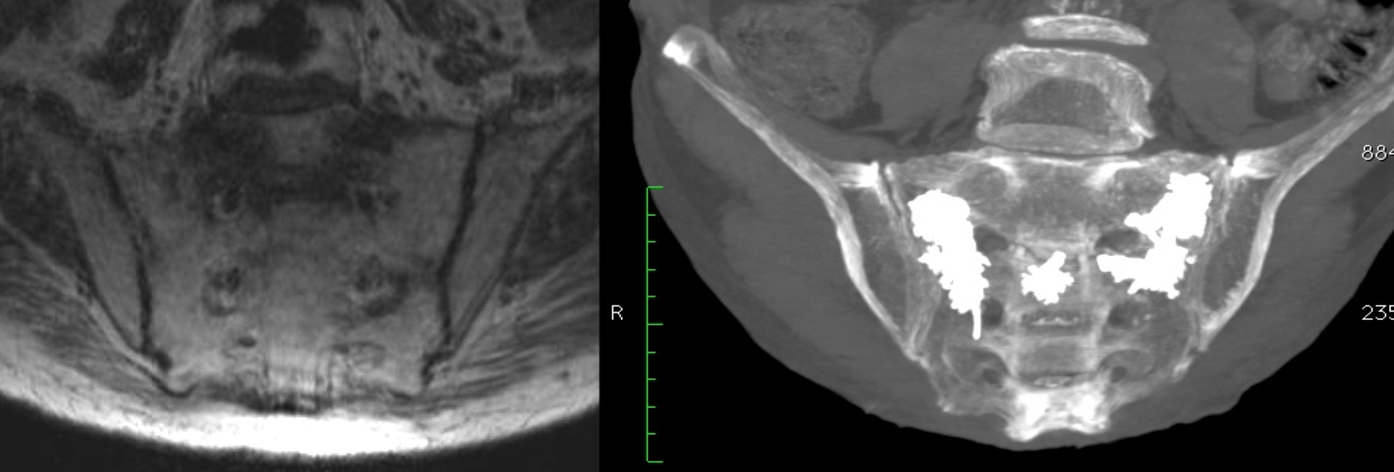
Example
Reconstruction of the sacral bone in bilateral "H" vertebral fracture. The MRI examination shows the fracture of the sacrum with the separation of the sacral wings from the body and interruption of the S2 soma. After introduction of the polymer, clearly evident in the image on the right in white, disappearance of pain with fusion of the sacrum and restoration of normalcy.
In some cases the vertebral fracture causes a collapse of the vertebral body, with consequent deformation of the vertebra itself, which loses its regular morphology to become a "wedge" structure, with consequent biomechanical alterations of the vertebral column (increase in kyphosis, muscle pain and articular from deformation of the column). If the physiological vertebral repair processes and the creation of a bone callus (usually therefore within 20-30 days at most from the fracture date) have not yet started, it is possible to raise the wedge vertebra by restoring the regular morphology of the vertebra itself, with the advantage not indifferent not only to the morphology of the fracture site vertebra, but to the posture of the entire spine.
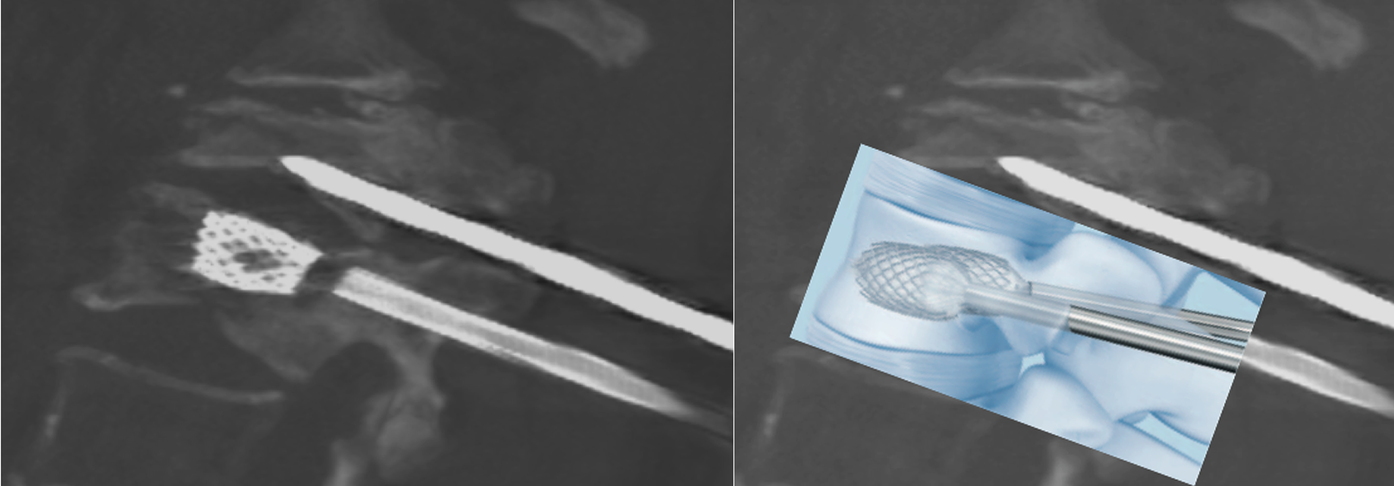
Among the various techniques in use, mention should be made of vertebral intrasomatic stenting, which consists, during a normal vertebroplasty procedure and always under local anesthesia, to open a cuboid-shaped titanium basket (stent) inside the deformed vertebral body which allows the vertebra to expand properly.
Example of vertebral stenting during percutaneous guided CT Vertebroplasty.
Example 1
Among the most successful and most promising modern techniques, the introduction of new biomaterials, with physico-chemical characteristics more similar to human bone, which allow to guide (osteoconductive) or stimulate (osteoinductive) the regrowth of the missing bone, for a more natural fracture repair close to the physiological mechanisms of bone healing. These new substances, already partially on the market in the main European countries, including Italy, constitute the new goal of vertebral fracture repair techniques.
Examples of bone regeneration using Osteoconductors (hydroxyapatite crystals) with bone regeneration..
Example1
MAGNIFICATION IMAGES TO THE ELECTRONIC MICROSCOPE OF THE NEW BIOMATERIALS
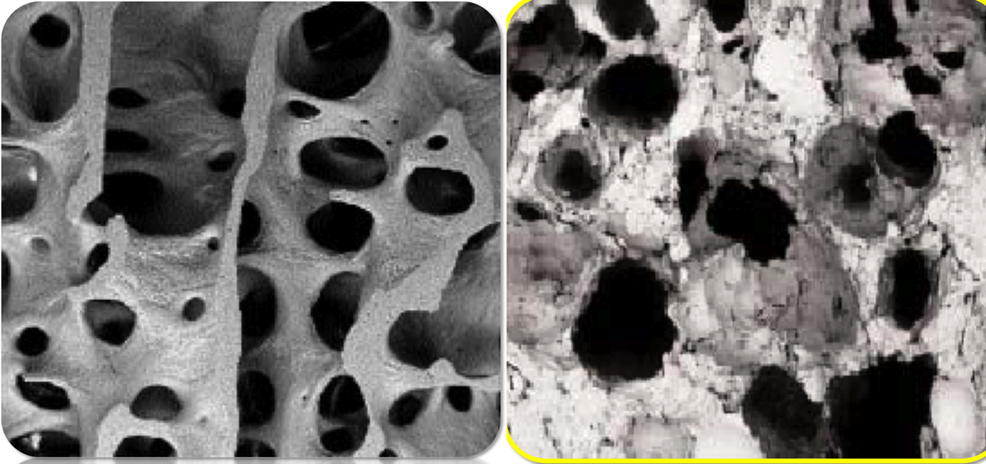
Human hydroxyapatite crystals (the bone scaffold) - Injected synthetic hydroxyapatite crystals

Vertebra before treatment - Introduction of crystals (arrow) - Sclerosis for bone regrowth at one month
No general anesthesia, no risk of deep scars, reduced surgery and hospitalization times.
LEARN MORE+
